Treatment options for testicular cancer
The following types of treatment are used:
Surgery
Surgery to remove the testicle (inguinal orchiectomy) and some of the lymph nodes may be done at diagnosis and staging. Tumors that have spread to other places in the body may be partly or entirely removed by surgery.
After the doctor removes all the cancer that can be seen at the time of the surgery, some patients may be given chemotherapy or radiation therapy after surgery to kill any cancer cells that are left. Treatment given after the surgery, to lower the risk that the cancer will come back, is called adjuvant therapy.
Radiation therapy
Radiation therapy is a cancer treatment that uses high-energy x-rays or other types of radiation to kill cancer cells or keep them from growing. External radiation therapy uses a machine outside the body to send radiation toward the area of the body with cancer.
Chemotherapy
Chemotherapy is a cancer treatment that uses drugs to stop the growth of cancer cells, either by killing the cells or by stopping the cells from dividing. When chemotherapy is taken by mouth or injected into a vein or muscle, the drugs enter the bloodstream and can reach cancer cells throughout the body (systemic chemotherapy).
See Drugs Approved for Testicular Cancer for more information.
Surveillance
Surveillance is closely following a patient's condition without giving any treatment unless there are changes in test results. It is used to find early signs that the cancer has recurred (come back). In surveillance, patients are given certain exams and tests on a regular schedule.
High-dose chemotherapy with stem cell transplant
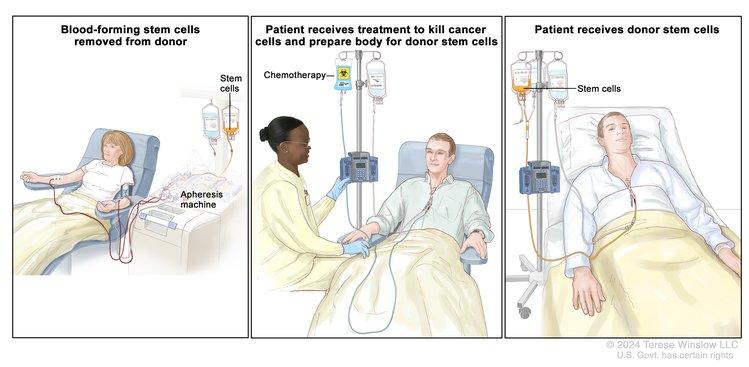
Stem cell transplants help restore blood-forming stem cells in people who have had theirs destroyed by certain cancer treatments.
Credit: © Terese Winslow
High doses of chemotherapy are given to kill cancer cells. Healthy cells, including blood-forming cells, are also destroyed by the cancer treatment. Stem cell transplant is a treatment to replace the blood-forming cells. Stem cells (immature blood cells) are removed from the blood or bone marrow of the patient or a donor and are frozen and stored. After the patient completes chemotherapy, the stored stem cells are thawed and given back to the patient through an infusion. These reinfused stem cells grow into (and restore) the body's blood cells.
See Drugs Approved for Testicular Cancer for more information.
Side effects of treatment
Treatment for testicular cancer may cause side effects. For information about side effects caused by treatment for cancer, visit our Side Effects page.
Treatment for testicular cancer can cause infertility
Certain treatments for testicular cancer can cause infertility that may be permanent. Patients who may wish to have children should consider sperm banking before having treatment. Sperm banking is the process of freezing sperm and storing it for later use.
Clinical trials
For some patients, taking part in a clinical trial may be the best treatment choice. Clinical trials are part of the cancer research process. Clinical trials are done to find out if new cancer treatments are safe and effective or better than the standard treatment.
Many of today's standard treatments for cancer are based on earlier clinical trials. Patients who take part in a clinical trial may receive the standard treatment or be among the first to receive a new treatment.
Patients who take part in clinical trials also help improve the way cancer will be treated in the future. Even when clinical trials do not lead to effective new treatments, they often answer important questions and help move research forward.
Patients can enter clinical trials before, during, or after starting their cancer treatment
Some clinical trials only include patients who have not yet received treatment. Other trials test treatments for patients whose cancer has not gotten better. There are also clinical trials that test new ways to stop cancer from recurring (coming back) or reduce the side effects of cancer treatment.
Clinical trials are taking place in many parts of the country. Find clinical trials for testicular cancer at Treatment Clinical Trials for Testicular Cancer. Clinical trials supported by other organizations can be found on the ClinicalTrials.gov website. Information about clinical trials is available from the NCI website.
Follow-up care
As you go through treatment, you will have follow-up tests or check-ups. Some tests that were done to diagnose or stage the cancer may be repeated to see how well the treatment is working. Decisions about whether to continue, change, or stop treatment may be based on the results of these tests.
Some of the tests will continue to be done from time to time after treatment has ended. The results of these tests can show if your condition has changed or if the cancer has recurred (come back).
Men who have had testicular cancer have an increased risk of developing cancer in the other testicle. A patient is advised to regularly check the other testicle and report any unusual symptoms to a doctor right away.
Long-term clinical exams are very important. The patient will probably have check-ups frequently during the first year after surgery and less often after that.