What is inflammatory breast cancer?
Inflammatory breast cancer is a rare type of fast-growing breast cancer in which cancer cells block lymph vessels in the skin of the breast. In the United States, 1%–5% of all breast cancers are inflammatory breast cancer. Most inflammatory breast cancers are invasive ductal carcinomas, which means they develop from cells that line the milk ducts of the breast and then spread beyond the ducts.
What are risk factors for inflammatory breast cancer?
Inflammatory breast cancer is more common in certain age groups and populations. Inflammatory breast cancer is:
- often diagnosed at a younger age
- more common and diagnosed at a younger age in Black women than in White women
- more common in women with obesity than in women at a healthy weight
The cause of inflammatory breast cancer is unknown, and other risk factors are the same as for other types of breast cancer. For more information, visit Breast Cancer Causes and Risk Factors.
What are the symptoms of inflammatory breast cancer?
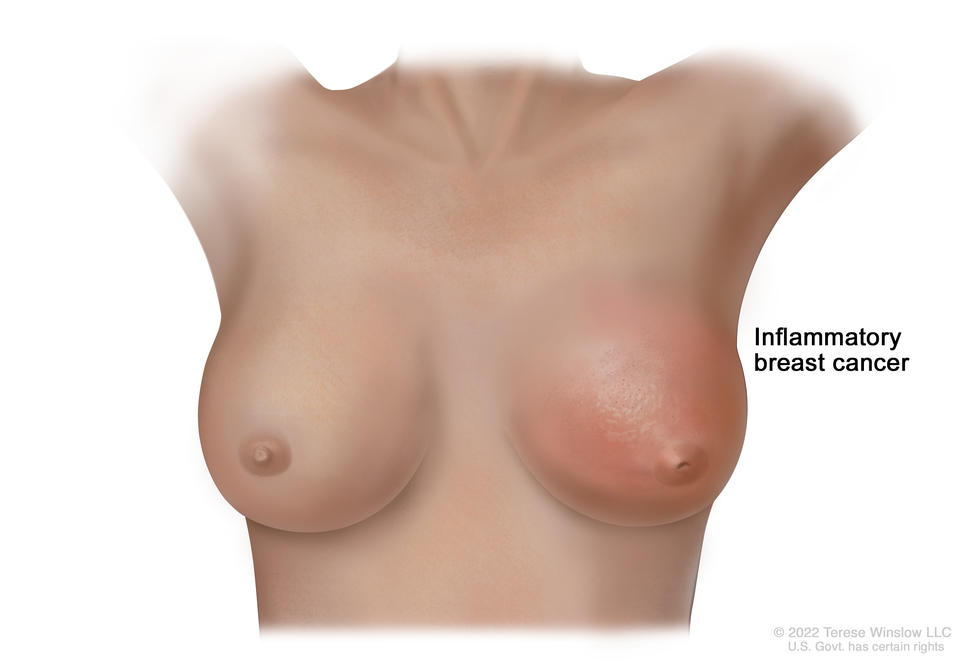
This type of breast cancer is known as inflammatory because it causes the breast to become red and swollen, or inflamed. Inflammatory breast cancer usually does not form a lump you can feel. Symptoms of inflammatory breast cancer include:
- pink, reddish purple, or bruised appearance of the skin of the breast
- dimpling or ridges on the skin that resemble an orange peel, caused by the buildup of fluid (lymph) in the skin of the breast
- rapid increase in breast size
- sensations of heaviness, burning, or tenderness in the breast
- a nipple that is inverted (facing inward)
- swollen lymph nodes under the arm or near the collarbone
These symptoms generally come on rapidly. They may also be signs of other diseases or conditions, such as an infection, injury, or another type of breast cancer that is locally advanced. Mastitis is an infection of the breast that has symptoms similar to those of inflammatory breast cancer. Mastitis can occur in anyone, but it is particularly common among people who are breastfeeding. If you have any of these symptoms, contact your doctor for evaluation.
How is inflammatory breast cancer diagnosed?
Because inflammatory breast cancer may develop and progress quickly, often between regular screening intervals, mammograms and other screening methods are less effective at diagnosing it early. Also, inflammatory breast cancer usually cannot be seen on a mammogram.
If you have symptoms of inflammatory breast cancer, your doctor will need to find out if they are due to cancer or another condition. Your doctor may:
- do a physical exam, including a clinical breast exam
- ask about your personal and family medical health history to learn more about your symptoms and risk factors for breast cancer
- do imaging tests, such as a mammogram, breast ultrasound, or breast MRI
- do a breast or skin biopsy
If it is cancer, additional tests may include:
- Biomarker tests. These will check the cancer cells for hormone receptors and HER2 protein that may help plan treatment. Inflammatory breast tumors are often hormone receptor negative. Learn more about Tests for Breast Cancer Biomarkers.
- PET scan or CT scan. These imaging tests will determine the extent of spread of the cancer.
Your doctor will assign a stage to the cancer based on a combination of the extent of spread, hormone receptor and HER2 status, and other tumor features, such as tumor grade. Inflammatory breast cancer is either stage III (stage 3) or stage IV (stage 4) when diagnosed, depending on whether cancer cells have spread only to nearby areas or to distant tissues as well.
Learn more about tests used to diagnose breast cancer and the different stages of breast cancer at How Breast Cancer Is Diagnosed and Breast Cancer Stages.
How is inflammatory breast cancer treated?
Because inflammatory breast cancer grows quickly and is more likely to come back after treatment, you may receive more treatment for a longer period of time than people with other types of breast cancer.
For information about how inflammatory breast cancer is treated, visit Inflammatory Breast Cancer Treatment.
What is the survival rate and prognosis for people with inflammatory breast cancer?
Doctors estimate inflammatory breast cancer prognosis by using statistics collected over many years from people with the disease. One statistic that is commonly used in making a prognosis is the 5-year relative survival rate. The 5-year relative survival rate tells you what percent of people with the same type and stage of breast cancer are alive 5 years after their cancer was diagnosed, compared with people in the overall population.
Inflammatory breast cancer tends to have a less favorable prognosis and survival rate than many other types of breast cancer because it is often diagnosed at an advanced stage and grows and spreads more quickly. Your doctor is in the best position to discuss your prognosis with you. Some people like to have a loved one or friend with them for the conversation.
Five-year relative survival rates among women with inflammatory breast cancer (note that there is no localized category for inflammatory breast cancer):
- 53% among women with regional inflammatory breast cancer (cancer has spread beyond the breast to nearby lymph nodes or organs)
- 22% among women with distant inflammatory breast cancer (cancer has spread beyond the breast to a distant part of the body)
To learn more about factors that affect breast cancer prognosis, visit Breast Cancer Prognosis and Survival Rates.
Ongoing research will increase our understanding of how inflammatory breast cancer begins and progresses, which could lead to new treatments and better outcomes for women with this disease. If you have been diagnosed with inflammatory breast cancer, you may want to talk with your doctor about the possibility of participating in a clinical trial. Learn more about clinical trials at Cancer Clinical Trial Information for Patients and Caregivers.