FDA Approves First Therapy for High-Risk Neuroblastoma
, by NCI Staff
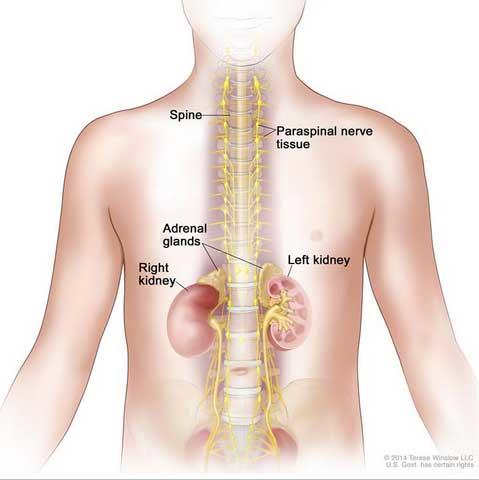
Neuroblastoma may be found in the adrenal glands and paraspinal nerve tissue from the neck to the pelvis.
The Food and Drug Administration (FDA) has approved dinutuximab (Unituxin™) as part of first-line therapy for children with high-risk neuroblastoma—the first approval of a therapy specifically for patients with the high-risk form of this disease. The FDA approval covers the use of dinutuximab after first-line multiagent, multimodality therapy (i.e., surgery, chemotherapy, and radiation therapy) for patients who have at least a partial response to this initial treatment.
Neuroblastoma is a cancer of immature nerve cells. It is the most common solid tumor cancer in childhood, with approximately 700 cases occurring in the United States each year. Approximately one-half of these cases are classified as high risk. Even with aggressive treatment, only 40 to 50 percent of patients with high-risk neuroblastoma survive the disease.
Dinutuximab is a monoclonal antibody that binds to a molecule known as GD2. This molecule, a ganglioside (a complex molecule that contains both lipids and carbohydrates), is expressed on the surface of neuroblastoma cells. Binding of dinutuximab to GD2 initiates an immune response that can kill the cells.
The FDA approval was based on the findings from an NCI-sponsored phase III clinical trial conducted by the Children’s Oncology Group (COG) and led by Alice Yu, M.D., Ph.D., of the University of California, San Diego. The pivotal clinical trial focused on 226 children with high-risk neuroblastoma who had responded to initial treatment.
Patients were randomly assigned to receive either an oral retinoid drug, isotretinoin (RA), or RA plus dinutuximab in combination with two immune-boosting compounds, interleukin-2 (IL-2) and granulocyte-macrophage colony-stimulating factor (GM-CSF). Three years after treatment assignment, 63 percent of participants receiving the dinutuximab combination were alive and free of tumor growth or recurrence, compared to 46 percent of participants treated with RA alone. Overall, 73 percent of participants who received dinutuximab in combination with IL-2 and GM-CSF and RA were alive compared with 58 percent of patients who received RA alone.
The most common serious adverse reactions seen in the clinical trials of dinutuximab include infections, infusion reactions, low blood pressure, and pain. The FDA approval comes with a boxed warning for infusion reactions and neuropathy. Almost 20 percent of patients in the dinutuximab arm discontinued treatment because of side effects.
NCI played several critical roles in dinutuximab’s clinical development. In addition to conducting the initial preclinical studies on the drug, NCI manufactured it through the Biopharmaceutical Development Program at NCI-Frederick because the drug was not being developed by a private-sector company when the phase III trial was launched.
After randomization to the phase III trial was stopped in 2009 because of the efficacy of the dinutuximab regimen, NCI provided dinutuximab to clinicians treating children with high-risk neuroblastoma under a COG-led expanded-access clinical trial.
Between 2009 and 2014, approximately 700 children received NCI-manufactured dinutuximab through this program, explained Malcolm Smith, M.D., Ph.D., associate branch chief of pediatrics in NCI’s Cancer Therapy Evaluation Program. Safety data from these patients was included in the dinutuximab application to FDA. Through this experience, COG researchers identified ways to manage some of the serious side effects associated with this treatment regimen, Dr. Smith noted.
In 2010, NCI entered into a Cooperative Research and Development Agreement with Maryland-based United Therapeutics Corp., under which the company assumed responsibility for manufacturing dinutuximab and moving it through the steps required for regulatory approval. As part of the dinutuximab approval, United Therapeutics will conduct additional studies to gather more information about the product's safety, efficacy, and optimal use.
NCI’s role in developing dinutuximab provided an important bridge until a commercial partner could step in and take responsibility for moving dinutuximab through FDA approval, Dr. Smith stressed.
“Children with neuroblastoma will benefit from this collaboration,” he said. “And importantly, it provides a pathway for future development of agents for childhood cancers, even when there is no pharmaceutical company initially interested in them because there is no adult indication.”