
Inside Cancer Careers Podcast: Season 1, Episode 4
In this episode of Inside Cancer Careers, we hear from Dr. Adrienne Boire, a Physician Scientist at Memorial Sloan Kettering Cancer Center, discuss how being a clinician in the research world is like Alice in Wonderland. We then hear from Dr. Jim Woodgett, a President and Scientific Director of the Terry Fox Research Institute, Canada, Senior Scientist at the Lunenfeld-Tanenbaum Research Institute (LTRI), and Professor in the Department of Medical Biophysics, University of Toronto, who shares his career in cancer kinases from the point of view of a scientist, institute director, and head of a funding organization.
Find this episode on YouTube.
Episode Guests
Segment 1: A Lab Tea Party
Adrienne Boire, M.D., Ph.D.
Adrienne Boire, M.D., Ph.D. is the Geoffrey Beene Junior Faculty Chair at Memorial Sloan Kettering Cancer Center in New York. As a neuro-oncologist, she cares for patients with metastasis to the central nervous system (CNS), with particular focus on leptomeningeal metastasis. As a scientist, she runs a laboratory-based research program focused on leptomeningeal metastasis. Her team employs multi-omic analysis of human samples to identify cancer cell adaptations to the challenging microenvironment of the leptomeninges. Leveraging mouse models, in vitro modeling, and classical biochemical techniques, the team uncovers the mechanistic implications of these discoveries to understand the biology of the leptomeningeal space and establish novel therapies for leptomengingeal metastasis.
In this episode, Dr. Adrienne Boire talks about how being a clinician in the research world is like Alice in Wonderland.
Segment 2: A Career in Cancer Kinases

Jim Woodgett, Ph.D.
Jim Woodgett is a President and Scientific Director of the Terry Fox Research Institute, Canada, Senior Scientist at the Lunenfeld-Tanenbaum Research Institute (LTRI) and Professor in the Department of Medical Biophysics, University of Toronto. After completing his PhD in biochemistry from the University of Dundee with Professor Philip Cohen in 1984, he pursued postdoctoral studies at the Salk Institute under Professor Tony Hunter and in 1987 returned to the UK to establish an independent research group at the Ludwig Institute for Cancer Research, London, UK where he isolated and characterized genes for several regulators of key signaling pathways including the stress-activated proteins kinases, PKB/Akt and GSK3. In 1992 he moved to the Ontario Cancer Institute in Toronto where his lab focused on signaling mechanisms underscoring malignant growth, degenerative diseases and diabetes. He then moved to the LTRI at Mount Sinai Hospital in 2005 where he served as Director of Research for 15 years. A significant fraction of his 300+ publications concern the biology and functions of a protein termed GSK3, which was a topic of the last chapter of his PhD thesis, highlighting the long time-lines often associated with pursuit of fundamental biological science.
Show Notes
Segment 1: A Lab Tea Party
Ad: NanCI by NCI mobile application
Segment 2: A Career in Cancer Kinases
- Dr. Jim R. Woodgett
- Ludwig Cancer Research
- Lunenfeld-Tanenbaum Research Institute
- Terry Fox Research Institute
Your Turn: Guests Recommendations
Episode Transcript
[UPBEAT MUSIC]
OLIVER BOGLER: Hello and welcome to Inside Cancer Careers, a podcast from the National Cancer Institute. I'm your host Oliver Bogler. I work at the NCI, in the Center for Cancer Training.
On Inside Cancer Careers we explore all the different ways that people join the fight against disease and hear their stories.
Today we are talking to Dr. Adrienne Boire a physician scientist at Memorial Sloan Kettering Cancer Center about how being a clinician in a research world is like Alice in Wonderland, and Dr. Jim Woodgett of the Lunenfeld-Tanenbaum Research Institute who shares his experience on cancer research from the point of view of a scientist, institute director and head of a funding organization.
Listen to the end for recommendations from our guests and to hear how you can send us yours in a segment we call “Your Turn”.
OLIVER: It's a pleasure to welcome Dr. Adrienne Boire to the show. Dr. Boire is an associate member of Memorial Sloan Kettering Cancer Center in New York City. She's a physician-scientist who treats and studies brain metastases, and I met her at a conference where she gave a really intriguing talk on lab culture, which we'll get to in a minute, but Dr. Boire, welcome.
ADRIENNE: Thank you. It's lovely to be here.
OLIVER: And I wanted to start with your journey. I'm always fascinated to learn how people come to do the work that they do, and I wonder if you'd be willing to share that with us?
ADRIENNE: Oh, sure. Yes, I think my path to becoming a physician-scientist is certainly not a traditional one. I grew up in Minnesota, and was always a curious kid, but truthfully, I thought that when I was going to college, that I might become a diplomat. I really enjoyed foreign languages. I enjoyed the idea that, you know, through listening, and kind of considering all of the possibilities that we could ultimately find ways to compromise. And, you know, I was an idealist, so, you know, come to world peace, right? But when I was in college, I was taking a biology class, a biochemistry class, and we were hearing a -- we were hearing about the Krebs cycle for the first time, and it was a transformative event for me, as unbelievable as that sounds, because I know quite a lot of people don't love biochemistry. So we were hearing about, you know, the just the basic processes that underlie molecular life, and I thought it was just gorgeous. I mean, it still is gorgeous. It still gives me goosebumps. It still kind of inspires me actually, this idea that the, you know, the biochemistry is really the grammar of life, right? And I think that was sort of my entry into all of biology, into becoming a scientist, was this idea that I really wanted to understand kind of the grammar of life. I really wanted to understand the rules that define how cells do what they do, how, you know, how cells are put together to make organs, how it all works together was just, and still is, utterly fascinating to me. So that's how I got hooked, and from then, actually, I spoke to the professor after that lecture, and basically asked him, "Do you know how cool this is? I can't believe that this is like -- that you just passed this by." I was kind of annoyed with my friends in class, who are taking notes because I thought, "How can you even take notes? This is far too fascinating to even -- you just had to appreciate it." And he said people like you would go to graduate school, and no one in my family had done anything close to that, so I followed his advice and applied to graduate school, and I did my PhD at Tufts University at the biomedical campus in Boston where I worked on a kind of an entomology and signal transduction project where we had found a new ligand for a receptor. So I was studying the protease-activated receptors, also known as the thrombin receptor, and we had found that actually a matrix metalloprotease can cleave the receptor productively and lead to signal transduction, and this was all in a context of cancer biology. And so while I was there, my mentor actually, Athan Kuliopulos, he was a physician-scientist, and I had truthfully never met a physician-scientist before. The physicians that I knew were the general practitioners who the, you know, the family practice doc who, you know, set my broken bones and delivered my brother. I'm from a small town, and I had never even encountered this kind of medicine before and even this kind of thinking. And I was intrigued, and I thought, well, these are my people, because they think in a really different way. They think, in terms of the organism and in terms of disease, but they also think in terms of mechanism, and I found that irresistible, and it is kind of a funky personality type, I think we can all agree. Physician-scientists are different people, and so --
OLIVER: How are they different? Now that you've said it, I have to ask.
ADRIENNE: I guess I think we are a little bit like scientific diplomats when I think about it, right? We kind of straddle these two worlds where we sort of view the same question in kind of, almost sort of like a chiral way, right? We see the same problem in opposite ways, and a physician-scientist has the capacity to see it as a physician and also see it as a scientist and to kind of toggle back between those two identities, and I think that kind of intellectual flexibility is key to the job, and also key to success as a physician-scientist, so --
OLIVER: Which explains why you gave the talk that we'll get to in a moment, but just to finish your story then, are you saying then you were in graduate school and decided to then also go to medical school afterwards?
ADRIENNE: I did, I did. So when my paper -- we were in our final revisions, and then I applied to medical school, and then went over to the University of Chicago for medical school. So and in medical school at UofC, you know, there are -- some schools tend to be kind of magnets for physician-scientists and I met so many physician-scientists in a wide variety of specialties, and I really -- I found a lot of commonalities and kind of a kinship with neurologists and neuroscientists, and so elected to pursue my clinical training in neurology, and did my neurology residency at Columbia. And then, in fellowship, I sort of put everything together. So I knew I wanted to study the brain. I knew that I loved cancer biology and mechanism, and I had been following Joan Massagué for many years, going to his lectures, reading his papers. I had sort of a science crush on him. I kind of -- I just loved his work.
ADRIENNE: And so I thought, I really want to study metastasis, and I couldn't think of really no better place to do that than with Joan Massagué at Sloan Kettering, and so, I sort of figured out where I wanted to do my scientific training first, and then from that, I thought this is where I will pursue my postdoc, and then I back-formed my clinical training to correspond with that, and I was fortunate that at Sloan, I would be doing my clinical training at a place where neuro-oncology was literally born, where the subspecialty of neuro-oncology was, was first sort of defined by Jerome Posner. So, I was able to study at the -- you know, elbow to elbow with these giants, and that was transformative for me. That's where I found leptomeningeal metastasis, which is the center of my scientific universe. It's where I first started appreciating ways in which we could study this disease from the perspective of a basic scientist, but also from the perspective of a physician, and it's the community that's really fostered my growth. I have a practice there now, where I treat patients with leptomeningeal metastasis. I run clinical trials, but the vast majority of my time is spent running my laboratory where we investigate the leptomeninges from soup to nuts. We look at how cancer cells live in the space, and we also look at the space itself, what, you know, what is the biochemical composition of the leptomeninges? What is the cellular composition? How does this change over time and under different stresses? Yeah, it's the best job ever. I have a terrific time doing my job.
OLIVER: Fantastic. Just a quick definition, leptomeninges, that's the lining of the cerebrospinal fluid cavity.
ADRIENNE: Yeah.
OLIVER: I probably didn't say that right.
ADRIENNE: Yeah.
OLIVER: Yeah?
ADRIENNE: No, you said it perfectly. So the leptomeninges are the kind of soft coverings of the brain and the spinal cord. So all of the meninges, these are all of the coverings, they're the pachymeninges or the dura, and the kind of outer hard kind of more rough coatings, and then the softer coatings are the leptomeninges, and they contain the circulating cerebrospinal fluid.
OLIVER: So it's the bag you keep your brain in, basically.
ADRIENNE: It's the bag that holds the brain, where the brain water is kept. It supports, and it also is one of the major interfaces between the brain and the systemic circulation. So it's also in many ways the front door to the brain. It's the way that the brain also can communicate biochemically with the rest of the body.
OLIVER: So you've mentioned the term physician-scientist several times. Obviously, it means a little bit of physician, a little bit of scientist, but what does that look like in practice?
ADRIENNE: So in practice, I never really take my physician hat off, because my patients are extraordinarily ill, but in day-to-day life, I run my laboratory, truthfully, seven days a week, I'm thinking about laboratory things. I don't think I could stop thinking about spinal fluid if you paid me, but I have clinic a half-day a week, and that half-day kind of spills over into a few other days because of course I'm answering patient phone calls. If my patients are in the hospital, I pop over to see them, but I'm a 90/10 physician-scientist, meaning that 90% of my effort is on the research side, and then 10% of my effort is on the clinical side.
OLIVER: So the continuous contact with patients informs the areas that you're investigating in your lab, I imagine.
ADRIENNE: Absolutely, so I have this privilege of being able to care for these patients and to take part in a pretty tense and extraordinary part of their lives, and this allows me to not just, you know, do the emotional work of caring for people, but it really provides me with a lot of hypothesis generation, which can sound sort of cold, but the way I mean it is, is that, you know, when I see how a disease unfolds in a human being, this necessarily provides me with a lot of unique observations and also some questions. So, for example, patients with leptomeningeal metastasis very often have seizures. And, you know, what is a seizure? Well, a seizure is an area of an extremely organized electrical activity on the surface of the brain. And normally, this is not the case, so why is this happening? Is there a metabolic cause for this? Is -- could the cancer cells be the nidus that's causing this metabolic cause that's causing this ultimate disorganization and this clinical outcome? So these are the sorts of things that I see at the bedside, that then kind of cause me to reexamine the way that I think about the process at the bench. My lab --the people in my laboratory are lovely people, and definitely are quite interested in the patients, and so very often I have a member of my laboratory at my side when we're seeing patients in clinic, and I'm surprised how often they are the ones who make the clinical observations, because very often, I'm trained to kind of just see patterns and to think about them in a clinical context, but the people in my laboratory, they'll say things like, "Well, what's happening there? Why is her finger twitching?" And I'll say, "Oh, that's because she's having a focal motor seizure." And then that precipitates this discussion. So I really love the way that I'm able to kind of bring the people in my laboratory to the bedside. And before COVID, truthfully, we don't do this so much anymore, because of COVID restrictions, but before COVID, patients and their families would occasionally come out to our laboratory or come to lab meeting, because they wanted to see how we conduct research, and because of course, we're using their patient samples, so we bring spinal fluid from the clinic into the laboratory to study. And I think that there are a lot of ethical difficulties with this process of really thoughtfully and carefully using patient samples, and I think the best solution is to be utterly transparent. So I talk to the patients and, you know, consent them of course, for the use of their samples, and we're very clear with them about what we're doing with the samples, what we can learn from the samples that we couldn't learn from our mouse models, and then what happens with their data? So is it -- you know, how is this -- is it de-identified? How so? And then where is it published? And I think that this process really allows everyone to derive a lot of meaning from what could be a pretty bleak complication of cancer. I think it's really lovely how generous my patients are, actually.
OLIVER: That's fascinating. Thank you so much. I can also see of course that being a physician-scientist gives you access to both cultures, and that's where I want to turn now. You gave this fascinating lecture, "Scientific diplomacy, everyone wins," so you kind of did become a diplomat, after all.
ADRIENNE: I did.
OLIVER: And in this lecture that you gave, this talk at the conference, you used a famous scene from literature to orient people to the culture that's often encountered in biomedical research teams, particularly from the viewpoint of the clinician. What scene did you pick and what gave you that idea?
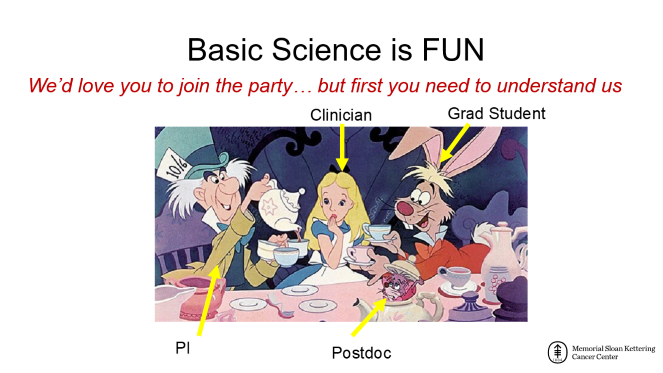
ADRIENNE: So I picked the tea party scene from Alice in Wonderland, and I chose it because actually, my husband used to teach literature and one of the books that he would teach is Alice in Wonderland by Lewis Carroll, and what I love about this scene and about Alice in Wonderland generally, is that I like that, you know, Alice in Wonderland, at first blush, it seems to be just kind of this kind of chaotic and almost kind of trippy experience, right, where you think nothing really makes sense, but of course, Lewis Carroll was a mathematician and really enjoyed logic, and when you take it down to its first principles, Alice in Wonderland is intensely logical. And that, I think, also spoke to me in terms of this clinician-scientist framework, that from the outside, it might seem that scientists are kind of goofy and silly, but we're actually very logical. We're very logical creatures, and so I thought that was a nice moment of an outsider coming into something that seems chaotic, but is not.
OLIVER: So our listeners may not be intimately familiar with the book, so what I thought I would do to orient them to the framing of your ideas was to give a brief summary and I asked ChatGPT to describe the scene, and I only edited what ChatGPT said a little bit, so let me read that and then I'd like to go further with your -- how you sort of disassembled the scene and to make it helpful. So here's what ChatGPT said. “The Mad Hatter's Tea Party is a famous scene from the classic novel Alice's Adventures in Wonderland by Lewis Carroll. The party takes place in a strange surreal world where everything is topsy-turvy and rules of reality don't seem to apply. Here's a description of the scene. Alice stumbles upon the Mad Hatter's Tea Party while wandering through Wonderland. The Mad Hatter, the March Hare and the Dormouse are seated at a large elaborate table, set with fine China, teapots and cakes. However, Alice is not invited to sit, so she is left standing awkwardly on the fringes of the party. The Mad Hatter and March Hare are engaged in a nonsensical conversation about time while the Dormouse dozes off at the table. Alice tries to join in the conversation but finds it impossible to follow the logic. The Mad Hatter then invites Alice to join in a tea party game, but it confuses her further. The party continues in a chaotic manner with the Mad Hatter and March Hare constantly switching seats and Alice trying to make sense of their strange behavior.” So in your analogy, who is Alice?
ADRIENNE: Alice would be the clinician, and the Mad Hatter is the PI, so is the principal investigator in a basic science laboratory.
OLIVER: Okay, and the Dormouse?
ADRIENNE: So the Dormouse is, you know, is a postdoc, so he's asleep in a teapot.
OLIVER: And the March Hare, I think was the graduate student.
ADRIENNE: The March Hare is the graduate student, exactly.
OLIVER: So tell us more about the these different roles and how you feel this diplomacy that you're proposing can help collaboration?
ADRIENNE: Sure. I think, you know, part of the reason that I bring this up is because I would think that what is essential to a real conversation, a real collaboration, is understanding, right, and that we all want to work together. The scientists and the clinicians, we all really do want to work together well, but we get bogged down in these issues, because we don't really understand each other. And I thought, well, all right, so the -- as you illustrated, this tea party was sort of rolling along before Alice showed up, and it continued on after she left, right? And the party, you know, has its own rules, and so it seemed to me that we really need to understand all of the aspects of the tea party, and we're going to be able to play along a bit better. And so in terms of the members of the tea party, I thought, well, you need to understand the Mad Hatter. So the PI, you know, the PI's job is to really keep the tea party moving, no matter what, right? He's continually making the party happen. He's obtaining funding for the laboratory, so a PI is writing grants. She's getting, you know, she's constantly working with the NIH and the NSF, shout out to my friends at the NIH. She's -- you know, knowing that funds from grants don't really cover the cost of all work, PIs are often talking to donors, and we're really assigning nearly every dollar is going to a project. A PI also needs to publish results, so we need to write papers, we're reviewing other manuscripts and we're traveling quite a bit to give lectures and attend conferences, and we're teaching graduate students. We're lecturing, we're grading, we're interviewing, we're on thesis committees. And in general, the PI very often is feeling a little bit underappreciated by clinicians and by society, and so it's kind of, as in Alice in Wonderland, the PI, the Mad Hatter is sort of buzzing along and is sort of answering sort of perfunctorily to Alice's questions because, you know, he has bigger fish to fry. He's got to pour tea. The graduate student, the March Hare, you know, we always say mad as a March hare, right, because the graduate student is just delighted to be there, right? And that really encapsulates how graduate students generally are feeling. They are thrilled to be invited to this party, and they are learning everything sort of all at once. They're eager-eager. They're learning all these bench techniques. They're learning analyses and how to cope with failure. They're learning how to manage their time and projects, and they're learning how to do a lot of just how-to science, right? We say like they're learning how to write scientifically. They're learning how to give a lecture. They're learning how to critically read and how basic science is generated, but they're also enthusiastic and they are perhaps not so cynical and so are very often, you know, ready to make this Nobel Prize winning discovery. They're -- just the enthusiasm from a graduate student is often what kind of drives a lot of people in the laboratory because it's so infectious. And then of course, once the graduate student becomes the postdoc, they turn into the Dormouse, who is exhausted and is, you know, in the tea party of course, has fallen asleep in the teapot. So a postdoc is very often, you know, characterized as sort of working to the point of exhaustion, right? The postdoc needs a big paper in order to be able to get their own lab and to become the Mad Hatter, right, to become -- to get their own little tea party going. So they're sort of working on the edge of what is known. A postdoc is very often designing new methods, designing, you know, new analytic approaches. They're reading almost more than anyone else in the laboratory, and they're learning how to cope with this idea of sort of intense competition. And they're also learning little bits, like how to manage a team, how to teach practical skills, and how to write a grant, and how to write a review article, and they tend to be quite anxious. They're underpaid, and they're very often tired of explaining to friends and family that they're not that kind of doctor, which, you know, of course, brings us to the clinician. And the reason I bring up Alice is that I think it's also important for the members of the tea party, the basic scientists, to understand Alice. So Alice is our clinician or clinician-investigator, right? So she wants transitional data -- translational data, rather. She'd like new therapeutic targets. She's seeing patients, and as a result, is very tired. She's constantly battling the EMR, the electronic medical record. She's constantly answering emails and phone calls. She's in clinic. She's on service. She's taking up slack from trainees who have something called work hours, which a finished -- you know, a fully trained clinician doesn't really have work hours. And she really doesn't have very much time for work that's not billable, so she has very little time for research as otherwise stated. So the role of Alice, you know, she, if she's running clinical trials, is also dealing with a lot of writing where she's writing revisions for her trial, protocol deviations. She's calling and conferencing with co-investigators, etc. She also needs to teach students. She needs to lecture. She needs to grade. She needs to interview, and she has to teach at the bedside. Importantly, though, Alice is accustomed to leadership, as she is in the story, right? In the story, Alice, you know, is used to things sort of going her way and people listen.
OLIVER: Right. She's the focal point, yeah.
>> And she's the focal point of the story. And clinicians also tend to be used to a certain amount of societal respect and deference because this is how the hierarchical system of the clinical world runs, and so this is another fundamental tension in the relationship, right, that Alice comes to the Tea Party, and is like, "Explain this to me. Get this done." And the Mad Hatter won't give her the time of day, because, you know, he's busy pouring tea.
OLIVER: You have this fascinating slide where you talk about speaking science to basic scientists and you really sort of put up almost paired sentences, if you will, or paired ideas of how the different -- the two different specialties, if you will, speak. I wonder if you could tell us a little bit more about that?
ADRIENNE: Of course. So, the Mad Hatter -- you know, as a scientist, we're trained rigorously through many, many years, to really take a complex system and to break it down into an observation and a question, to derive a hypothesis from the question. And from the hypothesis, then we turn to method, and the method itself is encumbered by statistics, and then ultimately, interpretation, right? And this hierarchy of thought, and this rigorous approach is time-tested, and it's something that you can almost -- I don't know a scientist that can be broken up at once we've learned how to do it, right? However, very often, clinicians will come to a basic scientist and will say -- you know, they'll come right to a method. They'll say I want to do this method on this, you know, on this sample. So, the example that I used in my lecture was from Highlights magazine, which I remember from my childhood, of Goofus and Gallant. And of course, Goofus, and Gallant, you know, they have -- they ultimately want the same thing, but Goofus does it in the way that you should not do it, and Gallant, you know, always gets things done properly. So the example I used was, you know, if Goofus says, "I want two more pancakes," and then Gallant says, "May I have another pancake, please?" And of course, we know that Gallant is the right answer. So Goofus would say, "I want to run proteomics on CSF," whereas Gallant would say, "We hypothesize that the CSF proteome changes after immune therapy." And then now that that actually says something to a basic scientist. It actually is -- there is a hypothesis there, there is a question, and it actually tells the basic scientist sort of where to start, and also allows the basic scientists to engage in the conversation. So that's really speaking the language of science, you know, from a clinical standpoint to a basic scientist.
Those are the things that are said, you know, overtly, but there's quite a lot that remains sort of unsaid as well, and I think that this is almost the heart of the issue. So a scientist wants to discover patterns that are common to all life, right? Whereas clinicians tend to be very excited to discover a subclassification of a disease. Let's see. A scientist really wants to discover a rule, right? We want to discover the grammar of life, right? Whereas a clinician tends to discover or more interested in exceptions or extraordinary cases. So this difference between the rule and the exception, this is something I run into quite a bit in my life. A scientist likes to relate findings to other fundamental processes, like wound healing or development. And a clinician wants to relate their findings to treatment or therapeutics, right? Scientists are generally not very happy unless they have a mechanism, and clinicians are actually okay if with understanding something on a level of phenomena as long as the patients are improving, right? And that's also a huge difference. So the literature they read is very different. Scientists read basic science journals, and so this fills their head and kind of their subconscious, right? Whereas clinicians are reading clinical journals, and so this is also sort of how framing how they view the world. And so I think these kind of unsaid ideas are also underlying this, this kind of difficulty with conversation and this difficulty of understanding one another.
OLIVER: Yeah, fascinating. Another thing that I found really -- that really hit home for me in your talk was the fact that the Mad Hatter, the basic scientist, lives in Wonderland, while Alice, the clinician, visits Wonderland. And you describe the constraints that these two different -- these two people have in pursuing their own goals, and they can constrain how they could work together.
ADRIENNE: Absolutely, and I think this is also -- this is the other issue, right? In diplomacy, we think about this also. We think about not just who the players are, and what languages they're speaking and their kind of motivations, but also what constraints are there that are preventing them from working together. And the basic scientist, you know, has very few kind of uncommitted personnel. There's really no free person in the lab who's just sort of, you know, able to do work that should just walk in, right? The clinical scientist, of course, cannot perform the experiments herself, because she also doesn't have any time to train and she doesn't have the right training to do the experiments. The basic scientist doesn't have very much slush, you know, meaning a lot of kind of uncommitted funds to be able to do projects that just sort of come out of nowhere. And the clinical scientist very often has funding, but the funding is from pharma, and that funding from pharma very often comes with considerable constraints on the use of those funds. In terms of just space, you know, a basic scientist very often doesn't have enough free bench space. The scientist, the clinical scientist doesn't really have enough, you know, time to work in the lab. The basic scientist very often cannot, however, usually access clinical charts or clinical data, and so that -- those data are not available to the -- to the basic scientist, whereas the clinical scientist, you know, has a hard time interpreting basic science data herself. There are a few points where actually the constraints are very helpful to each other. So a basic scientist needs to be the corresponding author on a manuscript. And of course, the clinical scientist needs to be the first author, so there's that moment where it's like a-ha!
OLIVER: It all comes together.
ADRIENNE: It's like Jack Sprat, right? And, as you said earlier, I think the really the fundamental problem also is that the basic scientist lives in Wonderland. This is where he makes his home, and this is where, you know, we're ultimately judged on Wonderland constraints, right? So if a basic scientist doesn't get publications, doesn't get grants, you know, you know, we're out of a job. Whereas a clinical scientist who doesn't get publications or grants can fall back on, as they say, (I say this in quotes) seeing patients. So she's really visiting Wonderland. She may elect to live there, but this tension between someone who is living in the space and someone who's just visiting, this is real and this is something that I hear from pure basic scientists very often, this idea that, you know, I just don't have time and I'm not willing to take the risk and the space and all of this working with someone for whom this is essentially sort of like a mad holiday, right? And I know that both groups really want the same things, right? We both want to work on a disease process, right? We both want to ultimately use our work to help others, but I do think that we can work together, but providing we understand each other a bit better. I think that clinicians can attempt to be a little bit more question-driven, can frame their queries in more scientific terms, and can of course, read their potential collaborators' work, attend lab meetings. And writing grants and reviews together, really is going to forge some of these bonds and really help illustrate to the basic scientists that they truly want to live in Wonderland, that they're really willing to buy into this process. I do think that scientists, however, can be more open to new viewpoints. They can be open to visitors to Wonderland. They can read their collaborators' work, and they can visit the clinic in the hospital to see the disease in question and to see and really try and understand the constraints that the clinician is under, and of course, potentially, this could be hypothesis-generating for the scientist as well. And I think really working together with this, with eyes open and really understanding each other has the possibility of really being really, I guess -- how to say this without sounding too sunny -- I mean, of course, I think it's going to be helpful for both groups, but I think really, something new is created in this in this dialectic, right? So when a clinician and a scientist are truly working together, you really get more than the sum of its parts because you're forging a third entity, right? And that's huge. That's what -- that's why I work in a place like Sloan Kettering, right? It's like, why I work in a place where we have the clinicians and the scientists together so closely is because it's so generative to do this.
OLIVER: Thank you so much, Dr. Boire. I mean, what you've shared with us and the vision and the framing you've provided us is incredible. A lot of institutions put clinicians and scientists together, but they don't invest in the diplomacy that could really help spark those fruitful collaborations, like you described, so thank you so much for joining us for this and really appreciate it.
ADRIENNE: Oh, it's my pleasure. Thank you for inviting me.
[UPBEAT MUSIC]
OLIVER: PubMed lists over 270,000 cancer papers published in 2022 – that is a staggering 750 papers every day. It’s great that cancer research is such an active field, but it makes finding the pubs that are critical to your work a challenge. What if you had an AI that paid attention to the papers you read and suggested others as they appear in PubMed? That is exactly what the NCI is building with an app called NanCI. With me to discuss NanCI are two members of the team that are creating NanCI: Chris Perrien of Blue Pane Studios and Duncan Anderson of Humanise.ai.
Chris, you’ve been building apps for NCI for over a decade. What is new about NanCI?
CHRIS: Fundamentally NanCI represents a shift in user experience – in the prior generation of apps people had to know where to look to find things. Now, they can find the information using AI agents. I think of NanCI as a friendly research assistant who makes suggestions and answers questions. Of course, it is early days, and NanCI is still learning from their users, but they will get better and better over time.
OLIVER: Duncan, you bring AI expertise to the project. Can you tell us what capabilities that brings to NanCI?
DUNCAN: NanCI is all about connecting scientists. Right now the focus is on connecting them to papers relevant to their interests, which NanCI does by matching vector representations of abstracts and looking at co-citations. If you tell NanCI that you find a group of papers interesting, by bookmarking them, the app will keep an eye on PubMed for you and suggest related publications. You can also share these folders with colleagues and export them to your reference manager. You can read the paper right there in NanCI, and follow any author to see when they publish preprints. Down the road we intend to help people network based on shared scientific and career interests. And much more – these are just some of the features of the app.
OLIVER: Thanks, Chris and Duncan. Right now NanCI is available in the Apple app store, and it will be coming to android later this year. Download it and give it a try! Your feedback on NanCI is very welcome – you can send that to us here at NCIICC@nih.gov.
It's an honor to welcome Dr. Jim Woodgett to the show. He's a senior investigator at the London Phil Tenenbaum Research Institute, part of Sinai Health in Toronto. An accomplished scientist, mentor and leader. He also participates in discussions about the state of science, the nature of biomedical careers and what's going on in the world on social media. Dr. Woodgett has seen academic science from many different angles, and we'll get to that in a moment.
But I want to start with asking you, what motivated you to become a scientist?
JIM: Ah, jeez, I mean, that's a -- it's -- you know, when you go back and think about this, your sort of vision of what initially got you started is often -- often changes over time, right. So I think it's because of reading so many student applications to graduate school where they talk about their inspiration. And, you know, my story was not that inspiring. It was -- it a came out of realization I was just interested in discovering new things rather than repeating things.
And that came from a Saturday morning job I used to have or a whole day job where I was working in a greengrocer in a little village. And I hated doing the same thing every day. And so, no, I don't want to do this. But -- so science was appealing. And then it just was a series of just -- this is an in the early 1980s, a series of things falling into place, some good, some bad, and you get sort of pushed in different directions and, at the time, don't necessarily realize what's going on, right.
A lot of students today maybe overthink what they want to do because often our ideas of especially science and research are quite different. They're sort of molded by what we see on TV or reading books or what have you, whereas, in fact, it's not usually like that. It's in some ways much more interesting but also very different. And so I wouldn't -- I wouldn't overthink it.
And going back, you know, I was inspired by lots of people. Science seemed to be the future, as it were. It is the future. And I was, I can't point at one particular thing. I must say, though, you know, again, reading letters or applications for graduates -- the graduate school, some people have some remarkable driven ambitions. And I do sometimes wonder whether or not if, you're that driven in a particular direction, science maybe isn't the thing for you because you really got to be open-minded.
[00:02:51] And that's the most important, open-minded and being creative. Those are the two key aspects, key qualities which will define success, I think, in scientific research.
OLIVER: You got started working on kinases as a grad student, right?
JIM: I did. Yes, I did.
OLIVER: Why kinases?
JIM: Why kinases. Oh, you should know better than that. What a question. I mean, there's -- at the time, we -- this is pre-genomics and stuff like that. And I was working in the lab of Phil Cohen at the University of Dundee in Scotland. And I'd been -- had gone directly to his lab based on studies, citations of work I'd been doing for a project as an undergraduate. And it seemed like kinases were kind of interesting because they gave us an idea of at the time, what insulin was doing.
And, of course, insulin's really important with diabetes and all that sort of stuff. And so when I finished those studies on glycogen metabolism for my PhD, I was fortunate to get a postdoctoral fellowship with Tony Hunter at the Salk Institute. It's just amazing. Going from Dundee to Salk Institute was a bit of a culture clash, I can say, as well as a welcome weather improvement or upgrade. And he worked on tyrosine kinases and is still working on tyrosine kinases.
And I spent three years in his lab, but I didn't work on tyrosine kinase because I worked on other protein kinases. And that's because the majority of kinases don't phosphorylate tyrosine. A lot of interesting ones do. But a lot of interesting genes associated with cancer are protein kinases. And that's from the perspective of cancer research. And it gets really exciting because a lot of the precision tools, the inhibitors and drugs are now targeting protein kinases like the EGF receptor, for example, in certain forms of lung cancer and breast cancer with HER2/neu.
So these drugs are incredibly -- they really are the future of cancer research insofar as they target specific molecular changes, which are specific to the tumor cells, unlike most chemotherapy -- therapeutic drugs, for example, which target the property of a tumor cell, which is to grow uncontrollably. But, of course, there are important cells in our body which do that normally, and they also get affected by these chemotherapy therapeutic agents. So when you're targeting a specific molecular mutation in a cancer, the side effects and off-target effects tend to be much less of a problem.
And so, therefore, these drugs are much better tolerated by patients. So I think that's -- that's when I first got in -- at the Salk Institute was when I first got interested in cancer research. And then I moved to -- I was offered a position at the Ludwig Institute for Cancer Research where we both crossed paths.
OLIVER: Indeed.
JIM: [Inaudible] Yeah. Many, many years ago when we both had hair and colored hair. And, you know, that was -- again, that was being directed by an amazing leader in the field, Mike Waterfield, who actually identified and sequenced the EGF receptor and also with Paul Stroobant, who sequenced the platelet derived growth factor which to another -- two amazing findings which linked together the fact that oncogenes, which were actually taken up by viruses, oncogenic retroviruses pulled out bits of human DNA.
And, in these cases, were the proteins associated with growth factor control my defense is why protein kinases for all this time is because they are components of signal transduction pathways. And the signal transduction pathways are those processes by which cells understand their environment, they -- how they transmit changes in the environment or inside them -- themselves. DNA damage, for example, triggers signal transduction cascades. And it's kind of there. So they're the control circuitry of the cell, and it kind of makes sense to me that you want to be -- if you want to understand how normal cells and cancer cells are working, you need to understand how they're controlled.
This idea that, if you want to control the cell, of course, you control the controlling elements has borne fruit again and again and again.
If we look at most drugs and not just in cancer therapies but, in most drugs, they target some elements of signal transduction. For example, antipsychotic drugs, mood stabilizing drugs, they're all affecting signal transduction, G protein signaling, for example. So I think that's -- it's a bit of a -- you and I can afford to look back over many years and justify why we've worked on particular areas.
But that's my rationale, which is I think it's planned out. And there's still tons to be done. That's why I still am excited by protein kinases.
OLIVER: Talking of which, what's the best part of being a scientist?
JIM: Oh. Everybody says, oh, you know, it's -- there's moments of discovery when you really just have to do an experiment, you see a result, and you're the first person to see it. You know, I -- in 30 whatever years, I think that's happened to me a handful of times. And, my goodness, I don't think that's enough to keep you going to work and writing grant applications. It is amazing when you do put some jigsaw pieces together and see a bit more of the picture and are able to describe and to, you know, elaborate on that.
That certainly is a driver. But I think -- I think what it is for me is it sort of it -- science really doesn't care about what we think. All right. I mean, there are a whole -- the world, the universe around us doesn't care what we -- how we interpret the world. The only people who care are, of course, we, are us because we want to try to understand and, therefore, hopefully avoid -- you know, generate better medicines, and better rocket fuel or whatever that science is contributing to.
And that -- I find that actually very hum -- not humiliating. It is humiliating sometimes.
OLIVER: Humbling.
JIM: -- when your experiments go wrong. But, yeah. But, really, it's a form of humility to remind you that, in fact, you're just -- it's your ideas. And I think that's, again, comes back to another element. I started off about how creativity is really, really important as a measure of potential success for research. Creativity means being able to see things slightly differently from somebody else. And we've -- there are a lot of scientists in the world, so they're thinking about the same sort of problems.
So you need to be able to look at things a little bit askew, a little bit from a different perspective. And we need to value that. And it's difficult to teach people. They've -- they've either got it or they haven't. And that doesn't mean that -- you know, again, you can be a scientist and make tremendous contributions and never discover something totally new. What you're doing is you're filling out the rest of the jigsaw puzzle. Right? And that's very, very important as well. But I think, you know, what the discovery to me is the most important part.
OLIVER: So, Jim, you also took on a couple of roles. You were the director of the Lunenfeld-Tanenbaum Research Institute for 15 years, if I counted correctly. It's an institute of 800 people, a budget of upwards of $90 million, publishes over 700 papers a year. So what was it like to take on that role? And what skills did you have to learn maybe that you didn't already have from your research experience?
Yeah. Actually, that comes back to a previous question you had about what do you like about science and research.
And what I like, and I think this is probably true as you get older, actually, and by older I mean as soon as you start your own research lab, you realize that, you know, you're, you quickly become outdated in terms of techniques. And so you rely on students and postdoctoral fellows and technicians and highly skilled people to be doing the actual experiments. And you end up writing the grants and helping with the papers and all that sort of stuff. So we all actually start doing this pretty soon.
But it's a form of -- what you're ending up doing is living science vicariously, right? And so being a research director, you've got to -- you've got to take pride in other people's abilities to do great science. And you try to build an environment where that is -- you enable that, where you can enable that. And, therefore, you can have impact, not just in your own research laboratory but in helping others to achieve things which you could never do yourself.
And I think that's -- that was particularly rewarding when you're trying to recruit a new scientist and it may be in a particular area of neuroscience or in cancer research or whatever, it's amazing when you do interview six or seven people, and they're just amazing.
It's -- they've got some great ideas. And you really want to hire them all, but you can't. You've got to pick one or two. But that's a really important decision, right. And you make that decision not necessarily on just what they've done but clearly their potential for doing it again and building out their own programs but also how they fit in with your environment and your culture. So those things are really important. Those are all elements that I enjoyed very much about directing research.
OLIVER: Now, you've also just recently now taken on a another role. You're the President and Scientific Director of the Terry Fox Research Institute, which funds over $10 million annually in cancer research across Canada and internationally. That sounds like a very different kind of responsibility. Can you tell us more about that.
JIM: So, actually, we spend -- we invest about $30 million a year. It depends. We've had -- but we've had a couple of bad years. So the fundraising and especially for most listeners following this, the podcast in the US, the Terry Fox Research Institute is -- fundraises based on a amazing feat from a young Canadian, Terry Fox, in 1980 who had osteosarcoma.
Had his leg amputated. But he was an athlete, and he decided to run a marathon a day across Canada. And he got to Thunder Bay, which is about halfway, just well over, actually, halfway in northern Ontario. And, unfortunately, the cancer metastasized. And he subsequently died the following year. But the legacy of that sort of brought the country together to be aware of cancer research.
And when he was getting his chemotherapy after his initial diagnosis and he saw so many kids suffering and wanted to do something about it. So that's basically where the funds come from, from annual runs every year from the communities and schools. So we support cancer research just like the NCI and NIH do. And it's -- again, seeing, supporting, and enabling others is what I get out of this role.
OLIVER: So you've been running a research lab for a while. I wonder if you could share with us what advice you give to the students and postdocs that are in your lab.
JIM: Well, there's all sorts of advice. I know the first piece of advice is get lots of advice, and get it from -- ask anybody because everybody will have different experiences. Everybody's circumstances are different, and that's good. You want to get different experiences during your training. That's really important.
It's a great way to see the world. So, you know, I did my PhD in Dundee and then, as I mentioned, postdoc in San Diego. Getting to see completely different systems with totally different people really helps broaden your mind. And so, in the UK, I did my PhD. So it was a three-year program. And when I went to the Salk Institute, I was younger than quite a few of the graduate students because, of course, the US system is as the undergraduate degree's often four years, and then the PhD -- well, now it's -- it spreads out to beyond five years in many cases.
So that's changed a little bit. So -- and, in Canada, it's very much like the US. But you are investing this amount of time, right, in doing research, especially if you want to continue doing research either in the private sector where there's lots and lots of opportunities or in the public sector in universities or research institutes or in other sectors as well. So it's -- you know, the fact is only you know what your real motivations are. And so it's -- you've got to find, you know, what tweaks your interests, what tweaks your interests, what makes sense to you.
And you're not going to replicate what somebody else has done, and you're going to find your own path. But there isn't a -- one path. Being open to new opportunities. I think that's the key advice I would give to people. Recognize that it's important to be patient and persistent but also to enjoy what you're doing. If you're not enjoying it now, it's -- it's like, you know, further flagellation isn't going to help.
OLIVER: Well, thank you very much, Dr. Woodgett, for spending time with us and sharing your insights. Really appreciate it.
JIM: You're welcome.
OLIVER: Now it's time for a segment we call Your Turn, because it's a chance for our listeners to send in recommendations that they would like to share. If you're listening, then you're invited to take your turn. Send us a tip for a book, a video, a podcast, or a talk that you found inspirational or amusing or interesting. You can send these to us at NCIICC@nih.gov, record a voice memo and send it along. We may just play it on an upcoming episode. Now I'd like to invite our guests to take their turn. Let's start with you. Dr. Woodgett.
JIM: What I like to do actually is and it's you got to be careful, but I like to dive into YouTube to look at old science programs and not just it’s not because of learning new things. It’s just realizing what was really fascinating to audiences 20, 30, 40 years ago. And you can find this you know, there is there are various BBC programs called Horizon, which I used to watch when I was growing up as a kid. And I think what it does is it sort of gives you a perspective and you can do the same with, you know, interviews of Richard Feynman and other well-known scientists.
OLIVER: Thank you so much. I really appreciate it. Dr. Boire, please take your turn.
ADRIENNE: So I'd like to recommend a book of poetry. So I really love Mary Oliver. So she's an American poet, and she's known for her poems that explore the natural world and the experience of being a human being. So I'm just going to read a poem that I particularly love. It's called Wild Geese. And it says:
You do not have to be good. You do not have to walk on your knees for 100 miles through the desert repenting. You only have to let the soft animal of your body love what it loves. Tell me about despair, yours, and I will tell you mine. Meanwhile, the world goes on. Meanwhile, the sun and the clear pebbles of the rain are moving across the landscapes, over the prairies and the deep trees, the mountains and the rivers. Meanwhile, the wild geese, high in the clean blue air are heading home again. Whoever you are, no matter how lonely, the world offers itself to your imagination, calls to you like the wild geese, harsh and exciting, over and over, announcing your place in the family of things.
I just love that poem because I love the way it captures how we all belong, right? We all belong in this world. And we all belong in this family of things, in biology. And I also think it speaks to science itself, right? We all belong. We just we need to find our place in it. And once you do, once you find that thing that you love, well, that's all you really need. You just have to follow it.
OLIVER: Thank you so much, Dr. Boire. That was a great recommendation.
[UPBEAT MUSIC]
OLIVER: That’s all we have time for on today’s episode of Inside Cancer Careers! Thank you for joining us and thank you to our guests.
We want to hear from you – your stories, your ideas and your feedback are always welcome. And you are invited to take your turn to make a recommendation we can share with our listeners. You can reach us at NCIICC@nih.gov.
Inside Cancer Careers is a collaboration between NCI’s Office of Communications and Public Liaison and the Center for Cancer Training.
It is produced by Angela Jones and Astrid Masfar and Edited by Janette Goeser.
A special thanks to Lakshmi Grama and Sabrina Islam-Rahman.
Join us every first and third Thursday of the month when new episodes can be found wherever you listen – subscribe so you won’t miss an episode. I'm your host Oliver Bogler from the National Cancer Institute and I look forward to sharing your stories here on Inside Cancer Careers.
If you have questions about cancer or comments about this podcast, email us at NCIinfo@nih.gov or call us at 800-422-6237. And please be sure to mention Inside Cancer Careers in your query.
We are a production of the U.S. Department of Health and Human Services, National Institutes of Health, National Cancer Institute. Thanks for listening.