Motixafortide May Improve Stem Cell Transplants for People with Multiple Myeloma
, by Elia Ben-Ari
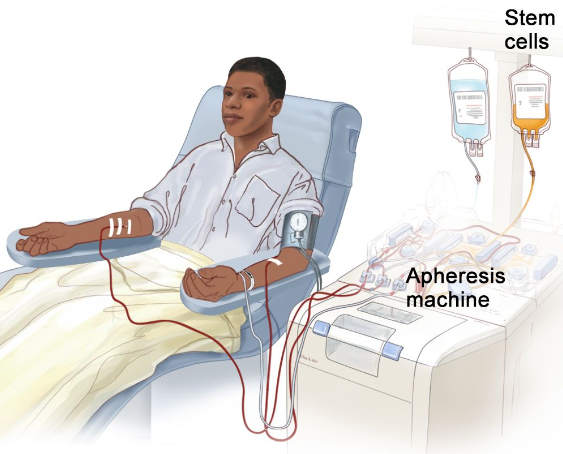
In a clinical trial, adding a single injection of motixafortide to G-CSF markedly increased the number of collected stem cells from people with multiple myeloma intending to undergo a stem cell transplant.
Credit: © Terese Winslow
UPDATE: On September 8, 2023, the Food and Drug Administration approved motixafortide (Aphexda) for use with filgrastim (G-CSF) as part of preparing for a stem cell transplant. The approval, based on the results of the phase 3 GENESIS clinical trial, is for people with multiple myeloma who will undergo a transplant with their own stem cells, known as an autologous transplant.
Details of the GENESIS trial are discussed in the story below.
For people with multiple myeloma, treatment often includes high-dose chemotherapy to destroy cancerous blood cells, followed by a stem cell transplant using cells collected from the patient’s own blood to aid recovery. But in about 15% to 30% of people who are fit enough for a transplant, the number of stem cells collected is not optimal for a successful transplant.
New clinical trial results show that an experimental drug could help overcome this problem. The drug, motixafortide, helps blood-forming stem cells move from a person’s bone marrow into their bloodstream.
In the trial, a single injection of motixafortide given in addition to a series of injections of G-CSF, the drug most widely used to “mobilize” stem cells from the bone marrow to the blood, markedly increased the number of collected stem cells compared with treatment with G-CSF alone.
Results of the randomized phase 3 clinical trial, which was supported by NCI and BioLineRx, the company that makes motixafortide, were published April 17 in Nature Medicine.
“These results are potentially practice changing because the drug is highly effective and easy to use,” said Eduard Schulz, M.D., Ph.D., of NIH’s Myeloid Malignancies Program, who was not involved in the trial.
If approved for this use by the Food and Drug Administration (FDA), the new drug could allow more people with multiple myeloma to collect optimal numbers of stem cells for their stem cell transplant while also speeding up and streamlining the collection process, said the trial’s lead researcher, Zachary Crees, M.D., of Washington University School of Medicine.
Transplanted stem cells help restore normal blood counts
In multiple myeloma, abnormal plasma cells (a type of white blood cell) build up in the bone marrow and blood and form tumors in bone. “Multiple myeloma is not curable, but long remissions are possible,” Dr. Schulz said. And high-dose chemotherapy and a stem cell transplant with the patient’s own cells, known as an autologous transplant, is one of the main ways to achieve a long remission, he said.
High-dose chemotherapy kills not only the cancer cells but also healthy stem cells (immature blood cells) in the bone marrow. To prevent patients from ending up with dangerously low blood counts, they then receive a stem cell transplant.
There are several steps to high-dose chemotherapy and autologous stem cell transplant. After the patient undergoes an initial treatment regimen (called induction) to reduce the amount of cancer in the body and induce remission, blood-forming stem cells are mobilized by different drugs and removed from their blood using a procedure called apheresis.
Then, after patients complete high-dose chemotherapy to kill any cancer cells that remain after induction treatment, their stem cells are returned to them through an infusion. The cells find their way to the bone marrow, where they start to produce new white blood cells, red blood cells, and platelets in a process known as engraftment. Patients remain in the hospital until their blood cell counts have recovered.
Getting an optimal number of stem cells for transplants
A transplant with less-than-optimal numbers of stem cells can delay or hinder recovery. “That can mean longer time in the hospital, increased need for blood transfusions, and an increased risk of infections,” Dr. Crees said.
It can also be “a big logistical and financial burden for patients,” especially if they live far from the transplant center, he noted.
Collecting fewer stem cells “also means that there aren’t any stem cells left over in case the patient needs them in the future,” Dr. Crees added.
Before collecting stem cells, doctors give patients treatments to get as many stem cells into the bloodstream as possible. Mobilization treatments include G-CSF alone, G-CSF plus certain chemotherapy drugs, G-CSF plus a drug called plerixafor (Mozobil), or a combination of all three drugs, Dr. Schulz said.
Patients may need multiple days of injections with G-CSF and plerixafor and multiple days of apheresis before enough stem cells can be collected—and even then, the number of cells may not be optimal for a rapid and reliable recovery, Dr. Crees said.
Improvements in transplant-related care have enabled older patients to safely receive stem cell transplants. However, older age and newer drugs or drug combinations used to treat multiple myeloma may impair stem cell mobilization, Dr. Crees and his colleagues wrote.
Small preliminary studies in people showed that motixafortide can dramatically increase the number of stem cells in the blood. So, researchers wanted to test it in a larger and more rigorous study of people with multiple myeloma, including older patients, who needed a stem cell transplant.
Safety, effectiveness of motixafortide
The GENESIS trial enrolled 122 people with multiple myeloma, ranging from 18 to 78 years old. Trial participants were randomly assigned to receive G-CSF plus motixafortide or G-CSF plus a placebo for stem cell mobilization.
The optimal number of stem cells for an autologous transplant is at least 5–6 million cells per kilogram of body weight, and “the bare minimum is 2 million per kilogram,” Dr. Schulz said. “Usually, engraftment and recovery of the blood cells is faster, and patients can leave the hospital sooner,” if they receive an optimal number of stem cells, he said.
In the trial, doctors were able to collect at least 6 million stem cells per kg in up to two apheresis sessions, done 1 day apart, from about 93% of patients treated with G-CSF plus motixafortide, compared with only about 26% of patients treated with G-CSF plus placebo.
Additionally, they were able to collect at least 6 million cells per kg after just a single apheresis procedure in 89% of patients who received G-CSF plus motixafortide, compared with 10% of patients who received G-CSF plus a placebo. The median number of stem cells mobilized in 1 day of apheresis was 10.8 million per kg with G-CSF plus motixafortide, versus 2.25 million per kg with G-CSF plus placebo.
“This is a huge difference, and potentially makes life better for the patient, who does not have to go through this [apheresis] process multiple times,” Dr. Schulz said. Limiting additional apheresis procedures and shorter hospitalizations could also reduce the cost of care, he noted.
But he cautioned that motixafortide’s cost, should it be approved by FDA, is still unknown.
BioLineRx has applied for FDA approval of the drug for use in mobilizing stem cells, with a decision expected by September.
Side effects of motixafortide, survival, and comparison with plerixafor
Overall, about 5% of patients in the placebo group and 28% in the motixafortide group experienced serious treatment-related side effects, but none were life-threatening. The most common side effects related to motixafortide treatment included short-lived pain and redness at the site of injection and temporary systemic (body-wide) reactions such as flushing, itching, or a feeling of warmth.
One year after transplantation, overall survival rates did not differ between the two treatment groups. The GENESIS team is continuing to follow participants to see if a survival difference emerges after longer follow-up.
The GENESIS study team also reported results from a small companion study comparing 14 patients treated with G-CSF plus plerixafor to a subset of participants from the randomized trial. Those findings suggest that G-CSF plus motixafortide is better at mobilizing stem cells than G-CSF plus plerixafor.
However, Dr. Schulz cautioned, this finding is not definitive because the two drugs were not tested head-to-head in a randomized trial. A randomized clinical trial comparing the drugs “would have been a better and fairer comparison,” he said, since plerixafor and motixafortide both work by blocking a chemical signal that tells stem cells to stay in the bone marrow.
Finally, Dr. Crees and his colleagues did a series of experiments looking at the different types of blood-forming stem cells mobilized by G-CSF plus placebo, motixafortide, or plerixafor.
“Not all stem cells are equal,” Dr. Schulz explained. And these experiments showed that motixafortide mobilized a higher percentage than plerixafor or placebo of the most primitive types of blood-forming stem cells, which could potentially lead to faster engraftment, he said.
Although high-dose chemotherapy with stem cell transplant plays a central role in the treatment of multiple myeloma, that may change as researchers continue to look for treatments that offer the possibility of longer-term survival or even a cure, including CAR T-cell therapy and other types of immunotherapy. And there is ongoing debate about how soon such therapies may replace or greatly reduce the need for autologous transplants, Dr. Schulz said.