Extensive Lymph Node Surgery Does Not Increase Survival in Melanoma
, by NCI Staff
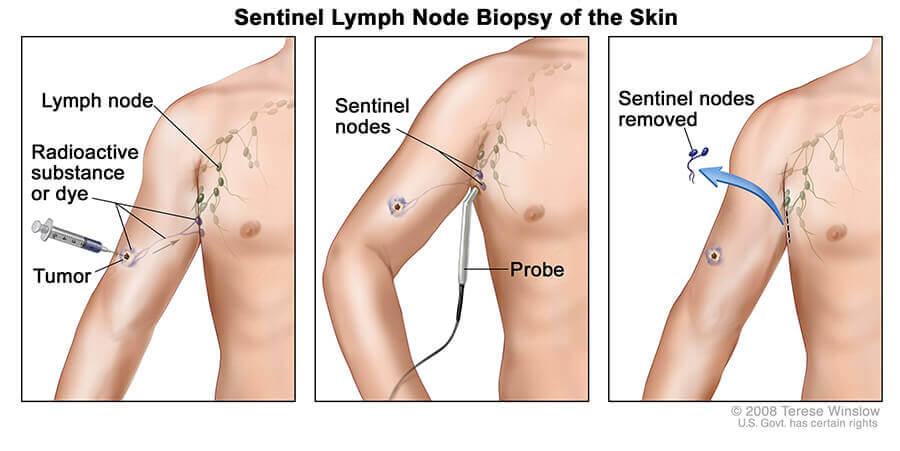
A sentinel lymph node biopsy of the skin.
Credit: © Terese Winslow
A conservative approach to lymph node removal surgery may be best for people with melanoma that has spread from the skin to one or a small number of nearby lymph nodes, new results from a large international clinical trial suggest.
In the trial, there was no difference in melanoma-specific survival between patients who had only the lymph nodes to which the cancer was most likely to spread, known as sentinel lymph nodes, removed and patients who had more extensive surgery to remove additional nearby lymph nodes.
Patients who underwent the more aggressive surgery, the trial showed, also had far more post-surgical complications.
The results of the second Multicenter Selective Lymphadenectomy Trial (MSLT-II), which was funded in part by NCI, were published June 8 in the New England Journal of Medicine.
“These results should be construed as practice changing,” Daniel Coit, M.D., of Memorial Sloan Kettering Cancer Center, wrote in an accompanying editorial.
“This is a very clear-cut, definitive result…that signals a turn in direction” for the care of people with melanoma, agreed Howard Streicher, M.D., of NCI’s Cancer Therapy Evaluation Program, who was not involved in the trial.
A Long-Standing Question
Most patients with newly diagnosed melanoma undergo a sentinel lymph node biopsy, in which the sentinel lymph nodes are removed and examined to find out if the cancer has spread from the skin. If the biopsy reveals melanoma cells in the sentinel nodes, doctors usually recommend immediate removal of the remaining regional lymph nodes.
“It seems logical to take those nodes out, even if we can’t detect melanoma there yet,” to keep the cancer from spreading, explained MSLT-II lead investigator Mark Faries, M.D., a surgical oncologist at the Angeles Clinic and Research Institute, an affiliate of Cedars-Sinai Medical Center, in Los Angeles.
But, until now, the survival benefit of this “completion” lymph node surgery had been unclear.
Participants in MSLT-II were 18–75 years old and had a skin melanoma of intermediate thickness (1.2 to 3.5 millimeters) that had spread to the sentinel lymph nodes but not to other parts of the body. (Tumor thickness is one factor that affects a patient’s prognosis.) Most patients in the study had one or two cancer-containing sentinel nodes.
Half of the 1,934 study participants were randomly assigned to have immediate surgery to remove the remaining lymph nodes in the area near the sentinel nodes (completion-surgery group). The other half were monitored with regular ultrasound exams to check for signs of cancer in these regional lymph nodes (observation group).
All participants had regular doctor visits with physical exams, laboratory tests, and imaging tests other than ultrasounds (such as PET scans or CT scans) that were standard for the center where they were treated, Dr. Faries said. The median follow-up time was 43 months, and some patients were followed for up to 10 years.
At 3 years, melanoma-specific survival was 86% in both groups—that is, 86% of the patients in each group had not died of melanoma. At 3 years, 68% of those in the completion-surgery group and 63% in the observation group had not experienced a recurrence.
The difference in disease-free survival, the study authors wrote, appears to be due to a reduction in recurrence of cancer in the lymph nodes after completion lymph-node surgery. No meaningful difference in the spread, or metastasis, of melanoma to other parts of the body was seen between the two groups.
Complications of surgery were more common in the completion-surgery group than in the observation group. At their most recent follow-up visit, 24.1% of patients in the completion group and 6.3% in the observation group had had lymphedema, a condition that occurs when excess lymph fluid builds up in tissues and causes swelling. Among all patients with lymphedema, the condition was mild in 64% of patients, moderate in 33%, and severe in 3%.
Remaining Questions
The MSLT-II investigators are continuing to follow study participants, Dr. Faries said, to monitor disease progression and deaths due to melanoma. They will also look for any additional long-term complications of the more radical surgery, such as nerve injury.
The findings to date “are definitive, unequivocal, and completely consistent…with the [recently] published results of one previous prospective, randomized clinical trial,” Dr. Coit wrote in the editorial. “The only remaining question is whether any patient with sentinel node-positive melanoma should undergo immediate completion lymph-node [surgery].”
Although Dr. Faries agrees that the study is practice changing, his view is that completion surgery “is no longer the sole ‘standard’ option for these patients.” More extensive surgery, he said, gives patients information about their prognosis that might influence their decisions about adjuvant therapy, treatment given after surgery to reduce the risk that cancer will come back.
Since 2015, a new adjuvant therapy option has been available for patients with stage III melanoma, and studies of other adjuvant treatments are ongoing. And “since the available therapies clearly have substantial pros and cons, the [prognostic] information may be worth the downside of [more extensive] surgery” to some patients, Dr. Faries said.
However, Dr. Streicher said, “if the disease has gone to the lymph nodes, the spread [of melanoma] probably has already occurred, prior to us being aware of the tumor and certainly before the surgery.” Researchers have found the same to be true in breast cancer, he noted, where “you don’t get better outcomes with more extensive surgery.”
Although patients who have a recurrence of melanoma in the lymph nodes may be able to have them removed at the time of recurrence, “many patients want to have the lowest risk of any recurrence possible, even without a survival advantage,” Dr. Faries said. “So, immediate completion surgery remains an option, but one that substantially fewer patients will choose with this new information.”
In the future, Dr. Streicher said, “we need to do better staging [of melanoma], and we need to better understand the biology of the disease, so that we know whom to treat with adjuvant therapy and who is cured by surgery.”